Watching someone you love lose control of their body — the tremors that won’t stop, the stiffness that locks the joints, the movements that happen without warning — is one of the most heartbreaking experiences a family can face. And when a doctor recommends Deep Brain Stimulation surgery, the hope is enormous. But so is the fear.
Deep brain stimulation recovery in India is a topic that thousands of patients and families research every year, often late at night, trying to understand what happens after the surgery, what to expect in the weeks that follow, and whether life will genuinely be better on the other side.
The honest answer is: for the right patient, DBS surgery is one of the most life-changing interventions in modern neurology. Not a cure — but a meaningful, lasting improvement that allows many patients to reduce medications, regain independence, and reclaim parts of life that Parkinson’s disease, essential tremor, or dystonia had taken away.
India has emerged as a globally trusted destination for DBS surgery — with experienced functional neurosurgeons, advanced neuroimaging and brain mapping technology, and a fraction of the cost compared to the USA, UK, or UAE. This guide will walk you through exactly what DBS recovery looks like, stage by stage, so you can prepare with confidence rather than fear.
What Is Deep Brain Stimulation (DBS)?
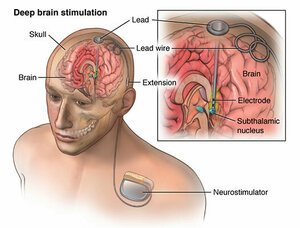
Deep Brain Stimulation is a surgical treatment in which a small electrode is precisely implanted deep within specific areas of the brain. This electrode delivers continuous, carefully calibrated electrical impulses that modulate abnormal brain activity — essentially interrupting the faulty signals that cause tremors, stiffness, and involuntary movements.
The system has three components:
1. The electrode (lead): A thin wire with four contact points implanted deep in the target brain region — most commonly the subthalamic nucleus (STN), globus pallidus internus (GPi), or ventral intermediate nucleus of the thalamus (VIM), depending on the condition being treated.
2. The extension wire: A connecting cable that runs under the skin from the head, behind the ear, down the neck to the chest.
3. The neurostimulator (IPG): A battery-powered pulse generator, roughly the size of a matchbox, implanted under the skin near the collarbone. This is the device that generates the electrical impulses.
DBS does not destroy brain tissue. It modulates — adjusts — the electrical environment. Because stimulation parameters can be changed wirelessly at any time by the neurologist, DBS is adjustable, reversible, and improvable over time. This adaptability is one of its most significant advantages over ablative brain surgeries.
Conditions Treated with DBS Surgery
Parkinson’s Disease
This is the most common indication for DBS globally. Parkinson’s disease causes a progressive loss of dopamine-producing neurons, leading to tremor, rigidity, slowness of movement (bradykinesia), and postural instability. DBS targeting the subthalamic nucleus or globus pallidus can significantly reduce these motor symptoms, particularly in patients whose medications are losing effectiveness or causing disabling side effects such as dyskinesias (involuntary movements).
Essential Tremor
Essential tremor is the most common movement disorder — causing rhythmic, involuntary shaking typically of the hands, arms, or head. When tremor is severe enough to interfere with eating, writing, or daily activities, and medications have been insufficient, DBS targeting the thalamus (VIM) can provide dramatic tremor reduction, often exceeding 80–90% improvement.
Dystonia
Dystonia causes sustained or repetitive muscle contractions resulting in abnormal postures and twisting movements. DBS targeting the globus pallidus internus is effective for primary generalized dystonia and cervical dystonia. Results in dystonia often take longer to appear than in Parkinson’s — weeks to months — but can be profound in well-selected patients.
Other Emerging Indications
DBS is also being studied and used in specialized centers for obsessive-compulsive disorder (OCD), treatment-resistant depression, and Tourette syndrome, though these represent a smaller, more specialized patient population.
Who Is a Good Candidate for DBS?
DBS is not appropriate for every patient with a movement disorder. Good candidates typically have:
For Parkinson’s disease:
- Diagnosis confirmed for at least 5 years
- Clear response to levodopa (L-DOPA) in the past — even if medications are now causing problems
- Motor fluctuations or dyskinesias that cannot be adequately controlled with medication adjustment
- No significant cognitive impairment or dementia
- No active psychiatric illness
- Realistic expectations about outcomes
For essential tremor:
- Tremor severe enough to significantly impact daily function
- Inadequate response to propranolol or primidone
- No significant cognitive decline
And For dystonia:
- Primary (genetic) dystonia generally responds better than secondary dystonia
- Young patients with generalized dystonia are often strong candidates
A thorough pre-operative evaluation — including neuropsychological testing, MRI brain, dopamine transporter (DAT) scan in Parkinson’s cases, and neurologist/neurosurgeon team assessment — determines candidacy. This evaluation is performed at all major DBS centers in India.
How DBS Surgery Works – Step by Step
DBS surgery at experienced Indian neurosurgical centers is performed in one of two ways:
Awake craniotomy technique (traditional approach): The patient is mildly sedated during the initial frame placement, then brought to an alert state during the actual electrode implantation. Being awake allows the neurosurgeon and neurologist to perform microelectrode recording — listening to individual neurons — and test stimulation effects in real time before finalizing lead position. The patient may be asked to perform simple tasks or report sensations. This sounds frightening but is generally well tolerated with appropriate sedation support.
Asleep DBS (intraoperative MRI or CT-guided): Increasingly available at advanced Indian centers, this technique allows the entire procedure to be performed under general anesthesia using real-time imaging for electrode guidance. It eliminates the patient’s need to be awake and is associated with comparable outcomes in experienced hands.
The procedure typically occurs in two stages:
Stage 1: Electrode implantation into the brain (bilateral, both sides, or unilateral depending on the patient’s condition). The skull is accessed through small burr holes using a stereotactic frame or frameless navigation system. Precise targeting uses high-resolution MRI planning and intraoperative confirmation.
Stage 2 (performed same day or a few days later): Neurostimulator implantation under general anesthesia — the pulse generator is placed under the collarbone and connected to the leads via an extension cable tunneled under the skin.
Total surgical time: 4–8 hours for bilateral DBS, 3–5 hours for unilateral.
Deep Brain Stimulation Recovery – Complete Timeline
This is the section patients and families need most. Recovery after DBS is not a single event — it is a staged process that unfolds over weeks and months, with genuine improvements continuing for up to 12–24 months as device programming is optimized.
Comprehensive DBS Recovery Timeline
| Time Period | What’s Happening | Symptoms Expected | Activity Level | Device Programming | Follow-Up |
|---|---|---|---|---|---|
| Day 0–1 | Surgery completed with ICU monitoring | Grogginess, headache, mild confusion | Bed rest | Device OFF | ICU monitoring |
| Days 2–4 | Brain swelling begins to settle | Fatigue, headache, temporary symptom improvement | Sitting up and short walks | Device may be switched ON lightly | Daily neurological checks |
| Days 5–7 | Discharge planning | Continued improvement and incision soreness | Light movement and walking | Initial low-level stimulation | Discharge with follow-up appointment |
| Weeks 2–4 | Wound healing and early adjustment | Variable symptoms with gradual adaptation | Gradually increasing activity | First formal programming session | 2-week wound check |
| Month 1–3 | Active programming phase | Progressive improvement as settings optimize | Increasing independence | Multiple programming sessions | Monthly visits |
| Month 3–6 | Settling into effective stimulation | Significant improvement in most patients | Near-normal or substantially improved function | Fine-tuning continues | Every 6–8 weeks |
| Month 6–12 | Long-term optimization | Continued gradual improvement | Full activity where appropriate | Maintenance programming | Every 3–6 months |
| Year 2+ | Stable long-term benefit | Sustained improvement with reduced medication | Full lifestyle engagement | Annual check and battery monitoring | Annual reviews |
First 24 Hours After DBS Surgery
The immediate post-operative period is spent in the neurosurgical ICU or high-dependency unit. Patients are carefully monitored for neurological status, blood pressure, and any early complications.
What to expect:
- Moderate headache — managed with IV pain medication
- Grogginess and fatigue from anesthesia and the length of surgery
- The stereotactic frame has been removed; the scalp incisions are small (typically 2–4 burr holes, each less than 1 cm) and covered with dressings
- The neurostimulator implant site near the collarbone is also sutured and dressed
- Some patients experience a phenomenon called the microlesion effect — a temporary but often dramatic improvement in symptoms in the first 24–72 hours. This is caused by mild tissue disturbance around the electrode and does NOT represent the device’s long-term benefit. It will fade as swelling resolves.
Family members are typically allowed brief visits during this period. Nursing staff closely monitor orientation, speech clarity, and limb movement to catch any early issues immediately.
First Week Recovery
By day 2 or 3, most patients are moved from the ICU to a general neurology ward. The improvement you may see in this first week is partly real, partly related to the microlesion effect, and partly from the light initial stimulation your neurologist may begin.
Key milestones in the first week:
- Most patients are sitting in a chair and taking short assisted walks by day 2–3
- The neurostimulator device may be switched ON at very low settings, allowing the brain to begin adapting to electrical stimulation
- Oral medications for Parkinson’s or other conditions are usually continued during this period
- Mild scalp tenderness and neck stiffness from the stereotactic frame positioning are normal and resolve within 1–2 weeks
- Discharge typically occurs between days 4–7 for uncomplicated cases
International patients are advised to plan accommodation in India for a minimum of 2–3 weeks after surgery to allow for the initial programming sessions and ensure travel is safe.
Recovery at 1 Month
The first month is a period of active adjustment. The neurostimulator settings are being progressively refined by your neurologist through repeated programming sessions. This process requires patience.
What patients commonly experience at 1 month:
- Variable day-to-day symptoms — some days are noticeably better, others more difficult
- Progressive reduction in tremor, rigidity, or dyskinesias as stimulation is optimized
- Fatigue is common and expected — the brain is adapting to an entirely new input
- Scalp wound is fully healed in most patients; sutures removed around day 10–14
- Many patients begin reducing Parkinson’s medications under neurologist guidance — a major goal of surgery
- Speech and balance may still be in flux; physical therapy begins providing measurable benefit during this period
It is important for families to understand that the first month is NOT when DBS shows its full benefit. Patience is essential.
Recovery at 3 Months
Three months is when many patients begin to understand what DBS can genuinely do for them. By this point:
- Multiple programming sessions have progressively found more effective stimulation parameters
- Many Parkinson’s patients have reduced their levodopa dose significantly — sometimes by 30–60%
- Tremor control in essential tremor patients is often excellent by this point
- Dystonia patients may be seeing early but meaningful improvements in posture and muscle control
- Energy levels have improved substantially
- Most patients are functionally independent for basic daily activities
- Physical therapy gains — improved balance, gait, and coordination — are consolidating
A formal motor assessment (using validated scales like the UPDRS for Parkinson’s) is typically performed at 3 months to objectively document improvement.
Long-Term Recovery Expectations
DBS is not a destination. It is an ongoing relationship between the patient, the device, and the neurologist. Over 6–24 months:
- Parkinson’s patients typically experience 40–60% improvement in motor scores
- Essential tremor patients often achieve 80–90% tremor reduction
- Dystonia patients may continue improving for 6–18 months after surgery
- Medication requirements are often substantially reduced, decreasing side effect burden
- Battery programming is periodically adjusted as the disease progresses or patient needs change
One realistic expectation to set: DBS does not stop Parkinson’s disease from progressing. It controls symptoms more effectively and for longer than medications alone. As the disease advances over years, stimulation parameters may need adjustment to maintain benefit.
When Does DBS Start Working?
This is the question every patient and family asks — and the answer requires honest nuance.
The microlesion effect (days 1–5): A temporary improvement from tissue disturbance around the electrode. Real, but temporary — don’t judge final outcomes by this.
Initial stimulation effect (weeks 1–4): As the device is switched ON and settings are adjusted, early benefits emerge — but at suboptimal parameters.
Meaningful therapeutic benefit (months 1–3): As programming is refined through multiple sessions, most patients experience significant, sustained improvement.
Peak optimization (months 3–12): Fine-tuning continues, often producing incremental improvements throughout the first year.
The honest answer: Most patients notice meaningful improvement by 3 months. Full benefit may take 6–12 months to realize.
Side Effects During Recovery
Understanding the difference between expected temporary effects and signs requiring medical attention helps patients and families navigate recovery with confidence.
Common Temporary Symptoms After DBS
| Symptom | Cause | Duration | Action |
|---|---|---|---|
| Headache | Surgery and frame placement | Days 1–7 | Pain medication and natural recovery |
| Fatigue | Anesthesia and brain adaptation | Weeks 1–4 | Rest and gradual activity increase |
| Mild Confusion | Post-anesthesia and brain swelling | Days 1–3 | Usually resolves without intervention |
| Scalp Tenderness | Incision healing | Weeks 1–3 | Normal healing and wound care |
| Neck Stiffness | Frame positioning during surgery | Days 1–7 | Physiotherapy and gentle movement |
| Variable Symptoms | Programming adjustment phase | Weeks 1–12 | Expected during device optimization |
| Tingling or Mild Speech Changes | Stimulation effect | Usually adjustable | Neurologist adjusts stimulation parameters |
Stimulation-Related Effects (Usually Adjustable)
One of DBS’s most important advantages is that stimulation-related side effects are generally correctable by adjusting the programming — changing voltage, pulse width, or electrode contact selection:
- Speech changes: Slurred speech or softened voice, particularly with bilateral STN DBS. Often improvable with programming adjustments or voice therapy.
- Tingling sensations (paresthesia): Common initially; usually resolves as settings are refined.
- Mood changes: Some patients experience transient euphoria or, less commonly, low mood. Manageable with programming and psychiatric support if needed.
- Double vision (diplopia): Usually stimulation-related and programmable.
- Balance changes: May temporarily worsen before improving as programming stabilizes.
Signs That Require Immediate Medical Attention
- Fever above 38.5°C (101.3°F) with incision redness or swelling — possible infection
- Sudden severe headache unlike previous headaches
- New weakness, numbness, or paralysis
- Seizures
- Sudden deterioration in level of consciousness
Serious complications are uncommon at experienced centers but require prompt evaluation.
Brain Swelling and the Healing Process
After any neurosurgical procedure, the brain experiences localized swelling (cerebral edema) around the implanted electrode. This is a natural healing response.
This swelling has two important effects:
- It causes the microlesion effect — temporary symptom improvement from the disruption of abnormal circuits, independent of stimulation.
- It temporarily masks the true stimulation effect — making it difficult to accurately program the device in the first 1–2 weeks.
For this reason, most experienced DBS teams perform definitive programming sessions after swelling has resolved — typically beginning serious optimization at 4–6 weeks post-surgery.
The swelling fully resolves in most patients within 3–6 weeks. Steroids may be prescribed post-operatively to manage swelling, particularly if the patient was awake during surgery and experienced prolonged microelectrode recording.
Speech, Walking, and Balance After DBS
These are the three functional areas that most concern patients and families — and all three deserve honest discussion.
Walking and gait: Most Parkinson’s patients experience improvement in gait — reduced shuffling, improved stride length, better ability to initiate movement — as stimulation is optimized. Freezing of gait (sudden inability to take a step) may improve, though it can be more variable. Physical therapy is an important complement to device programming for gait rehabilitation.
Balance: Balance typically improves as rigidity decreases and motor control normalizes. However, patients with significant pre-existing postural instability may not see dramatic balance improvement — this symptom is one of the less responsive to DBS. Physiotherapy focusing on balance training is strongly recommended.
Speech: Bilateral STN DBS carries the highest risk of speech-related effects — softening of voice (hypophonia) and occasional slurring. These can often be managed through programming. Unilateral DBS or GPi targeting has generally more favorable speech outcomes. Speech therapy is available at major Indian neurorehabilitation centers and is recommended when needed.
Device Programming and Battery Adjustment
Programming is not a one-time event. It is an ongoing, collaborative process between patient and neurologist that continues for months — and at regular intervals thereafter.
How programming works: The neurologist uses a wireless programmer to adjust stimulation parameters through the skin — no further surgery required. Parameters that can be adjusted include:
- Which electrode contacts are active
- Voltage (amplitude)
- Pulse width
- Frequency
- Stimulation mode (constant voltage vs constant current)
Programming sessions timeline:
- First activation: typically day 3–7 post-surgery, at low settings
- First major programming: 4–6 weeks post-surgery
- Active optimization phase: monthly or every 6–8 weeks for the first year
- Long-term maintenance: every 3–6 months, or sooner if symptoms change
For international patients: Shifam Health coordinates remote programming follow-up for international patients who return home after surgery. Your treating Indian hospital can conduct device interrogation and parameter adjustments via video consultation with a local neurologist. Remote programming systems from Medtronic and Abbott also allow some adjustments to be made from a distance.
Battery life: Most DBS neurostimulators last 3–5 years (rechargeable devices last longer — up to 15+ years). Battery replacement is a simpler outpatient procedure than the original surgery, performed under local anesthesia with a short recovery.
Physical Therapy and Rehabilitation After DBS
DBS surgery and physical rehabilitation are most effective when pursued together. Surgery addresses the neurological dysfunction; rehabilitation rebuilds the functional skills and physical conditioning affected by years of movement disorder.
Key rehabilitation components after DBS:
Physiotherapy:
- Gait retraining — improving stride length, speed, and safety
- Balance and fall prevention exercises
- Strength and flexibility work
- Teaching strategies to manage any residual freezing episodes
Occupational therapy:
- Fine motor skill retraining — handwriting, buttoning, utensil use
- Home environment assessment and modification
- Return-to-work planning
Speech therapy:
- Voice projection and clarity exercises
- Swallowing assessment if needed
- Strategies for communication if speech has been affected
LSVT BIG and LSVT LOUD: These are specialized rehabilitation protocols developed specifically for Parkinson’s patients. LSVT BIG targets large-amplitude movement, LSVT LOUD targets voice volume and clarity. Both are available at specialized rehabilitation centers in India and strongly recommended for Parkinson’s DBS patients.
Rehabilitation typically begins in hospital during the first week and continues as an outpatient program for 2–3 months. International patients can receive intensive rehabilitation during their India stay and continue with local programs at home.
Emotional and Mental Recovery
Brain surgery is not just a physical experience. The emotional journey of DBS surgery — before, during, and after — deserves the same attention as physical recovery.
Before surgery: Anxiety about brain surgery is universal and understandable. Detailed pre-operative counseling — provided at all major Indian DBS centers — helps patients and families understand exactly what to expect.
After surgery: Emotional adjustment takes time. Patients may experience:
- Transient elation: Particularly in the first few weeks, partly from relief, partly from stimulation effects.
- Mood fluctuations: As medications are adjusted, mood can fluctuate. This is expected and manageable.
- Adjustment to a new identity: For patients who have lived with severe tremor or rigidity for years, the experience of regaining control can be emotionally overwhelming — in a positive way. Adjustment takes time.
- Caregiver adjustment: Family members who have provided intensive care may need to adjust their role as the patient regains independence. This is a positive transition but can be unexpectedly complex.
Psychological support — individual counseling or support groups — is available at major Indian neurological hospitals and is particularly valuable during the first 3–6 months of recovery.
Lifestyle After DBS Surgery
Life after successful DBS surgery can be remarkably close to normal — and for many patients, more normal than anything they have experienced in years.
Activities that typically resume:
- Independent self-care — dressing, eating, personal hygiene
- Driving (after appropriate clearance — typically 6–12 months post-surgery in most countries)
- Light to moderate exercise, walking, swimming
- Social activities and travel
- Work return (depending on occupation — desk work typically 4–8 weeks, physical labor longer)
Activities requiring ongoing attention:
- Contact sports — not recommended due to risk of device damage
- Certain medical procedures (MRI — check device MRI compatibility with your center; therapeutic ultrasound — avoid near the device; electrocautery — requires specific precautions)
- Airport security — the device contains metal; patients carry a device ID card that explains this to security personnel
Ongoing relationship with your neurologist: DBS patients need regular follow-up for life — not because the treatment is fragile, but because programming optimization and battery monitoring are ongoing components of successful therapy. For international patients, Shifam Health coordinates this follow-up through a combination of in-person visits to India and remote telemedicine monitoring.
Can Patients Live Normally After DBS?
For most appropriate candidates, the honest answer is: yes — often far more normally than they have in years.
The best outcomes are typically seen in:
- Parkinson’s patients with good pre-operative levodopa response
- Essential tremor patients with classic limb tremor
- Young patients with primary generalized dystonia
Realistic expectations:
- DBS reduces symptoms; it does not eliminate them entirely in all cases
- Non-motor symptoms of Parkinson’s (such as memory changes, autonomic dysfunction, or depression) are generally not improved by DBS
- The disease continues to progress; ongoing neurological care remains important
- Regular programming and follow-up sustain the benefit over years
Many patients describe DBS as giving them their life back — the ability to eat independently, to write, to walk, to travel, to spend quality time with family without their condition dominating every moment.
DBS vs Medication Therapy – Comparison
| Aspect | Medication Alone | DBS Surgery |
|---|---|---|
| Tremor Control | Moderate and variable | Excellent, especially for essential tremor |
| Motor Fluctuations | Progressive worsening over time | Significantly reduced |
| Dyskinesias | Can be medication-induced | Often dramatically improved |
| Medication Dose | Often escalating | Usually reduced significantly |
| Medication Side Effects | Cumulative with higher doses | Reduced as medication dose decreases |
| Adjustability | Fixed through daily dosing | Fully programmable |
| Duration of Benefit | Often wanes over years | Sustained long-term with programming |
| Suitability | All patients initially | Selected patients after adequate medication trial |
| Reversibility | Fully reversible | Device removable with reversible brain effects |
Success Rate of DBS Surgery in India
At experienced Indian neurosurgical centers, DBS outcomes are comparable to published data from leading international institutions:
Parkinson’s disease:
- 50–60% improvement in motor UPDRS scores
- 30–60% reduction in total levodopa daily dose
- 70–80% improvement in tremor
- Significant improvement in dyskinesias in patients with this as a primary complaint
Essential tremor:
- 80–90% tremor reduction
- Most patients regain ability to perform precise tasks (writing, eating, drinking)
Dystonia:
- Primary generalized dystonia: 50–80% improvement in dystonia rating scales over 6–12 months
- Cervical dystonia: 60–75% improvement
Procedural safety at top Indian centers:
- Serious surgical complication rate: less than 2–3%
- Infection rate: approximately 1–3%
- Hardware malfunction: less than 2%
- Significant neurological deficit: less than 1%
India’s top DBS centers have collectively performed thousands of DBS surgeries, with volume directly correlating with the precision and safety of outcomes.
Also Read:
Gamma Knife Surgery for Epilepsy and Brain Disorders in India
Risks and Complications
Informed patients make better decisions. Acknowledging risks honestly is part of building genuine trust.
Surgical risks:
- Intracranial hemorrhage (bleeding in the brain): less than 1% at experienced centers — the most serious potential complication
- Stroke: very rare, less than 0.5%
- Infection: 1–3%, requiring device removal in severe cases
- Seizures: uncommon, typically manageable
Hardware-related risks:
- Lead migration or fracture: requires surgical correction
- Device malfunction: rare with modern hardware
- Skin erosion over hardware: uncommon
Stimulation-related effects (generally manageable through programming):
- Speech changes
- Balance or walking changes
- Mood changes
- Tingling or sensory effects
What patients should know: The risk profile is generally acceptable given the significant functional benefits for appropriately selected patients. An experienced multidisciplinary team — neurologist, neurosurgeon, neuropsychologist, and rehabilitation specialist — working together optimizes patient selection, surgical precision, and post-operative management to minimize complications.
Recovery Tips for Patients and Families
For patients:
- Follow wound care instructions precisely — keep incision sites dry, watch for signs of infection
- Take all prescribed medications consistently — do not stop Parkinson’s medications abruptly
- Attend every programming session — these sessions are where the real optimization happens
- Keep a symptom diary — noting which symptoms improve, which persist, and any new effects helps your neurologist program more effectively
- Be patient — DBS optimization is a marathon, not a sprint
- Start gentle physical activity early — short daily walks from week 2 onward
For caregivers:
- Provide support without taking over — encourage independence as the patient’s function improves
- Attend programming sessions where possible — understanding what the neurologist is adjusting helps you support the patient at home
- Watch for mood changes — emotional lability in the first few months is common and should be communicated to the neurology team
- Coordinate with Shifam Health for telemedicine follow-up after returning home — don’t let geography interrupt the programming process
Cost of DBS Surgery in India
One of the most significant reasons international patients choose India for DBS surgery is the dramatic cost difference compared to Western countries.
DBS Surgery Cost in India – Full Breakdown
| Component | Cost Estimate (INR) | Cost Estimate (USD) |
|---|---|---|
| Unilateral DBS (1 Side) – Indian Device | ₹4–6 lakh | USD 4,800–7,200 |
| Unilateral DBS (1 Side) – Imported Device | ₹6–9 lakh | USD 7,200–11,000 |
| Bilateral DBS (Both Sides) – Indian Device | ₹7–10 lakh | USD 8,400–12,000 |
| Bilateral DBS (Both Sides) – Medtronic / Abbott | ₹10–16 lakh | USD 12,000–19,000 |
| Rechargeable DBS System (Imported) | ₹14–20 lakh | USD 17,000–24,000 |
| Surgeon / Neurosurgeon Fees | ₹1–2 lakh | USD 1,200–2,400 |
| ICU / Hospital Stay (5–10 Days) | ₹1.5–3 lakh | USD 1,800–3,600 |
| Pre-operative Evaluation (Complete) | ₹40,000–80,000 | USD 480–960 |
| Rehabilitation (2–4 Weeks Inpatient) | ₹60,000–1.5 lakh | USD 720–1,800 |
India vs Global DBS Cost Comparison
| Country | Bilateral DBS Cost (Approx.) | Wait Time |
|---|---|---|
| India | USD 12,000–19,000 | Immediate |
| USA | USD 80,000–150,000+ | 2–6 months |
| UK (Private) | GBP 60,000–100,000 | 3–12 months |
| UAE | USD 35,000–60,000 | 2–6 weeks |
| Turkey | USD 18,000–30,000 | Immediate |
| Singapore | USD 35,000–55,000 | 2–4 weeks |
India offers comparable outcomes to the USA and UK at approximately 15–20% of the cost — with no waiting time for surgery.
Best Hospitals for DBS Surgery in India
The following hospitals have established functional neurosurgery programs with dedicated movement disorder teams and DBS expertise:
Delhi NCR:
- All India Institute of Medical Sciences (AIIMS), Delhi — India’s premier neuroscience institution, with a dedicated movement disorders program and extensive DBS experience
- Medanta – The Medicity, Gurugram — JCI-accredited, internationally recognized functional neurosurgery department with intraoperative MRI capability
- Fortis Memorial Research Institute, Gurugram — dedicated DBS program with experienced movement disorder neurologists
- Apollo Hospital, Delhi — established functional neurosurgery unit, strong international patient support
- Max Super Speciality Hospital, Saket — experienced neuromodulation team
- Institute of Brain & Spine (IBS), New Delhi — specialized neurosurgical center
Mumbai:
- Kokilaben Dhirubhai Ambani Hospital — advanced neuroscience center with functional neurosurgery expertise
- Hinduja Hospital — experienced neurology and neurosurgery team
Chennai:
- Apollo Hospitals, Chennai — one of the highest volumes of neurosurgical procedures in South India
- SIMS Hospital — growing neuroscience department
Also Read:
Top 10 Best Deep Brain Stimulation Surgery Hospitals in India : Updated List in 2026
What to look for:
- Dedicated functional neurosurgery or movement disorders program
- Neurosurgeon with subspecialty fellowship in functional/stereotactic neurosurgery
- Movement disorder neurologist for programming
- Intraoperative imaging capability (MRI or CT)
- Neurophysiology monitoring during surgery
- Post-operative rehabilitation program
- International patient services
Why International Patients Choose India for DBS
International patients selecting India for DBS surgery consistently cite the same factors:
World-class expertise without the wait: India’s top DBS centers operate programs that rival leading neuroscience institutions globally. And unlike the UK’s NHS or Canadian public systems where wait times for DBS can extend to months, India offers scheduling within weeks.
Transparent, affordable costs: Total DBS costs in India represent 15–25% of equivalent procedures in the USA or Western Europe. For families in Bangladesh, Nigeria, Kenya, Yemen, or other countries where DBS is either unavailable or prohibitively expensive locally, India represents a genuinely accessible option.
Advanced technology: India’s premier DBS centers use intraoperative MRI, 3D brain mapping, microelectrode recording technology, and the full range of Medtronic, Abbott, and Boston Scientific neurostimulator systems — the same devices and imaging infrastructure used at top centers in the USA and Germany.
Multidisciplinary care: India’s best DBS programs involve neurologists, neurosurgeons, neuropsychologists, speech therapists, and physiotherapists working collaboratively — mirroring the multidisciplinary standard of care at international centers.
Accommodation and comfort: Major hospital campuses have associated patient residences or partner hotels within walking distance, making extended stays during the recovery and programming phase manageable for international families.
Medical Visa and Travel Support
International patients coming to India for DBS surgery require an Indian Medical Visa (M-Visa), which permits extended stays for medical treatment and allows one or two attendants to accompany the patient.
Typical documents required:
- Valid passport (minimum 6 months validity)
- Completed visa application form
- Hospital appointment confirmation letter
- Medical reports supporting DBS indication
- Proof of financial capacity
- Return travel plan
Processing time: 3–10 working days at most Indian embassies. Priority processing is available with a hospital urgency letter where medically justified.
For more Details refer to this guide:
How to get Medical Visa for India: A Complete Guide (2026)
Planning your India stay for DBS: International patients should plan for a minimum of 3–4 weeks in India to allow for:
- Pre-operative evaluation (3–5 days)
- Surgery and immediate post-operative stay (5–7 days)
- Initial recovery and first programming sessions (1–2 weeks)
- Safe clearance for international travel
Shifam Health coordinates the complete patient journey:
- Pre-travel telemedicine consultation with DBS specialists for eligibility assessment
- Medical report review and hospital recommendation
- Cost estimation and hospital appointment scheduling
- Visa invitation letter from the treating hospital
- Airport pickup on arrival
- Interpreter services (Arabic, Bengali, French, Swahili available)
- Hotel or hospital guesthouse accommodation near the treating hospital
- During-stay coordination for all appointments and family communication
- Post-return remote programming follow-up coordination
- Ongoing telemedicine support with the Indian neurology team
Conclusion
Brain surgery is one of the most significant decisions a patient or family will ever make. And when that surgery is Deep Brain Stimulation — a procedure that reaches into the deepest circuits of the brain to restore what a movement disorder has taken — the weight of that decision is enormous.
But thousands of patients who have been through DBS surgery in India will tell you the same thing: the fear before surgery was far greater than the experience itself. And the improvement afterward — the stilled tremor, the unlocked stride, the returned independence — was more than worth it.
Deep brain stimulation recovery in India is a process that unfolds over months, guided by skilled neurologists and neurosurgeons who have dedicated their careers to functional brain surgery. It requires patience, commitment to follow-up, and the right medical team. All of that is available in India — at a cost that makes this life-changing treatment accessible to patients who could never afford it elsewhere.
Shifam Health is ready to help you take the first step. Share your neurological reports, your MRI scans, and your medical history with our team. We will connect you with India’s leading DBS specialists, provide honest guidance on whether DBS is right for you, and support you through every stage — from your first consultation to the day you walk back through your front door with a life reclaimed.
FAQs About DBS Surgery in India
How long does DBS recovery take?
Most patients leave the hospital within 5–10 days and see major improvement within 3 months, with continued optimization over 6–12 months.
Is DBS surgery painful?
Patients usually experience mild headache or scalp soreness for a few days, which is controlled with medication.
When can patients walk after surgery?
Most patients begin assisted walking within 2–3 days and walk independently within the first week.
What are the side effects of DBS?
Temporary headache, fatigue, or mild speech changes may occur. Serious complications are rare at experienced centers.
Can DBS cure Parkinson’s disease?
No. DBS does not cure Parkinson’s but significantly improves symptoms and quality of life.
How successful is DBS surgery in India?
Top Indian centers report outcomes comparable to global standards, with major improvement in tremor and motor function.
Which hospitals are best for DBS in India?
Leading centers include AIIMS Delhi, Medanta, Fortis Memorial Research Institute, Apollo Hospitals, and Max Super Speciality Hospital.
How long does the DBS battery last?
Rechargeable batteries may last 15 years or longer, while standard batteries usually last 3–5 years.
Is DBS surgery reversible?
Yes. Doctors can turn off or remove the device if necessary.
How does Shifam Health support international DBS patients?
Shifam Health assists with hospital selection, medical visas, travel planning, teleconsultations, and post-return follow-up support.